Greg, now 5 years old, had a seizure last Friday. I’m writing this down as detailed as my memory will allow me so that I can refer to it in the future.
The Night Before
I was working late the night before (code release). I was in my room. I could hear Greg and Steve playing as Steve tried to get Greg upstairs to go to sleep. It was so late. Why can’t he ever put him down at his actual bed time? Greg came to my room a few times during the release (which ended at 9:45pm). So I know he went to bed at 9:30 at the latest. Greg was in good spirits and came to my room to say good night. What a sweet baby boy.
That Morning
The next day, Greg came to my room to cuddle with me as soon as he woke up, as usual. He seemed a bit warm, but it didn’t even occur to me to check his temperature (missed clue #1). Greg came downstairs with me. He went to the bathroom and I gave him some breakfast. He said he didn’t want breakfast; his tummy was too full. This is strange for him, but Cheerios and milk have been known to give him tummy aches, so I figured his baby body was now coming around to rejecting it (missed clue #2). I told him I was sorry, and that’s all there was to eat. “I don’t want to eat it” and I said “You don’t have to… but the cheerios ARE getting soggy.”
I have been trying to get some work done before I leave for work in an effort to shorten my commute (leave late, run into less traffic). This was only the second day I managed to do it. So, after leaving him to his food, I went to the kitchen table and kept working.
He came to the kitchen holding the bowl saying “I just had a little bit, not all of it.” I told him I was proud of him for trying and took care of his plate. Then I got him dressed, and left him playing with his Legos in the living room. I went back to the kitchen to work.
After a few minutes, I heard silence. I thought that was weird, but decided not to investigate. 15 or so min later, I shut down the computer and went to get him to go to school: he had fallen back asleep on the couch. I thought this was also strange (missed clue #3), but since I had only started doing this “work before you go” routine, I really had nothing to compare today to. It was perfectly possible that he would be doing this every day that we leave late: get comfy on the couch and sleep a bit more.
I put his shoes on as he slept in order to wake him up gently. He asked if he could bring his favorite blanket and keep sleeping in the car. “Of course you can, baby. Let’s go to school.”
We didn’t listen to any music on the way to school, and he dropped his tablet to the side pretty quickly after we got in the car (missed clue #4). He normally plays his game until at least 10 min before we get to school. This time he wasn’t interested, and he also didn’t ask for music. I had a lot on my mind, so I welcomed the quiet time to put my thoughts together.
When we got to school, he was his happy energetic self. He said hi to all his friends and he helped me put his lunch in the fridge. I gave him a big hug and a big kiss, and went off on my merry way.
The Call
I was at work, doing nothing particularly exciting, when I got a call from an unknown number. I have been getting a lot of those “You’ve won a Caribbean vacation” calls, and I like to pick them up so I can add the number to my “DON’T PICK UP” address book entry. I picked up the phone. Greg’s teacher is on the other end. She said Greg is fine, however he had thrown up all over his clothes and his shoes. Since he didn’t have a lot of clothes at school, she had to let him borrow another boy’s shoes and shorts. My mind immediately went to the stupid Cheerios: his baby body was REALLY rejecting them this time, but I bet he’s fine now that he’s thrown it up (missed clue #5). The teacher said that the vomit was mostly water but there was a lot of it.
She asked whether I would like to pick him up at the park (where everyone was about to go) or at school. I asked her if he could just go to the park and finish the day, I was sure he was OK. She said the policy was that if a child is sick, the parent must pick them up. I looked at the time: 10:52am. I looked at my screen: not doing anything I couldn’t stop doing right then and there. So there was the question: let him go to the park, or not?
Since I knew he was FINE, I expected that if he went to the park with his friends he would perk up and play, making it harder for me to peel him off the fun to go home, not to mention what a waste of my time it would have felt: if he’s FINE, then WHY am I picking him up??? What am I going to do? Work from home the rest of the day? What is HE going to do? Should I drop him off at my mother-in-law’s? You know, it’s best if he doesn’t go to the park. So I told her just that.
I told my coworker what had happened, and he said “Oh, Ina, kids throw up. What’s the big deal?” and I played the opposite argument just to be contrary “Kids don’t just throw up! Do YOU just throw up? Is that something you do???” He laughed and insisted in his point.
I walked to my car thinking what a waste it was to even come in today. What a waste of a commute.
Drove to the school and parked outside at a meter. Normally I would park in their lot in the back of the school, but this was going to be so quick, that I didn’t mind just parking it out front. I left my work computer bag in the front seat, my sun-roof open, and put a quarter in the meter for a whooping 15 minutes, of which I would only need 5, I was sure.
I walked towards the school while playing Candy Crush. I was so distracted I walked right by it…. came back and punched in the code.
Identifying the Seizure
I walked into the school to find it desolate. All the kids and teachers had gone to the park on such a nice day. Only the poor newbie aid (not Greg’s regular teacher) had stayed behind to wait for me.
I introduced myself, and she said she knew me. She made me nervous. She seemed nice, but I had never seen her wearing the school shirt. Who is she anyway? Does she work here? (yes, she did).
I asked where he was. She said he told her that he went to bed late last night, and he was tired. So she took out her nappy stuff and put him down to rest.
I walked into his classroom and found him lying on his side on the nappy mat with his blanket on. He was staring right out into the distance, and his hand was near his mouth. He has the habit of picking his upper lip with his fingers.
I said “hi baby!” and he didn’t respond. I didn’t think much of it. Sometimes I walk into the school and say hi, and he says “hi mami” without even looking at me.
I got closer and closer and gave him a kiss and kept saying hi. He was still not answering me and not looking at me.
The teacher was talking the whole time, but I can’t remember what she was saying. Maybe telling me again that he said he was tired, maybe calling his name. I do remember her saying “Gregory, respond, you are scaring me.”
I pulled up his upper body to sit him up. He was staring into space. I asked him what he was looking at, but I had already started to get scared.
I pulled him up on his feet. I remember his knees being bent, as he stood up. I held his hand and pulled him across the room to where he was staring out. By the time we reached the door, I realized he wasn’t looking at anything at all, and this must be a seizure. He had had one before, but I wasn’t there for it. It had been described to me as exactly THIS.
I immediately tried to pick him up and told the teacher I would be taking him to the hospital now. However, as I picked him up it was like dead weight. I had no idea how I was going to manage to put him in the car seat. Never mind that he might be really sick and I could get stuck in traffic while taking him in. Never mind I had no idea how to get to the hospital from where I was. None of those things crossed my mind. The thought was simple: I can’t get him in the car. I have to call 911.
The 911 call
I got my phone out of my back pocket (fortunately I had not left it in the car like I usually would when I pick him up the normal way). I dialed 911.
I sat him down on a kiddy chair and looked at his face. His eyes were looking up at the ceiling.
I have always thought I would be clear and concise when calling 911. People tend to ramble unnecessary information. I’ve always thought I would listen for questions and answer them as succinctly, quickly and clearly as possible. So I did just that.
{I requested the 911 recording, but have not received it yet, this is just from memory, which is faulty}
911: Where is your emergency?”
ina: 9999 Street name. I have a 5-year old who is having a seizure.
911: …
They had me repeat the address a couple of times. They asked me for my name and phone number. They repeated what I said about the 5 year old. They asked me a few more questions. At the same time, the teacher kept talking to me with things to say (doing that rambling stuff I said I didn’t want to do). At one point I could not hear 911 over the teacher and I had to stop and ask her to be quiet, then got back to 911 and asked them to repeat the question.
Sometime early in the call his body started to shake and jerk. I was holding his right arm with my left hand, while I held the phone with my right. The teacher was holding his left arm in place.
911 asked me repeatedly NOT to hold him down. “He’s on a chair! I have to hold him up so he won’t fall down.” So they asked me to put him on the ground. “In what position?” I asked. Face down. I tried doing that, but told them that he might choke on his own drool. They said to put him on his side. I tried, but I could hear gargling noises. It didn’t feel right, so I picked him up and put him face down on my lap in fetal position, such that the head would be facing down.
Greg started coughing and then throwing up green goo. This felt like went on for a long time. I could see his eyes rolling up in their sockets. I put my phone down on the floor next to me with speakerphone on.
I could hear the ambulance sirens. The teacher said she would go let them in. Good thing she had the presence of mind to do that. I had not thought about how they would get into the school. I was just holding Greg and talking to 911.
The EMT and ambulance
The EMTs arrived and immediately took him off my lap and put him face up, reclined at an angle. The shaking stopped shortly after and he started shivering.
The EMTs put an oxygen mask on him and started an IV of fluids. They asked me a few questions, but I don’t remember what they were. After just a little bit (time unknown) I called my husband to tell him what happened, and to stand by for hospital name.
The EMTs asked me where to go. I said Children’s Hospital, and the decision was made. I sent a text to my husband to meet us in the ER.
I was asked to pick up Greg and put him in the stretcher. Although he wasn’t responsive, he was definitely awake and disoriented. Kept pulling all the wires off of him and did not like it when we tried to strap him to the stretcher. I kept talking to him saying mommy loves him and it’s going to be OK. There was no sign of him noticing this.
We got on the ambulance and I started singing songs to him. There was no response. His eyes opened up wide and he started pulling at all the wires. He even managed to remove his IV from his arm. We held him down as best we could.
When we got to the hospital, I took a video of it. I wanted to show it to him later. The driver saw me and asked if I was the mom, and I explained I was recording the video for him. He asked me if I wanted him to turn on the ambulance lights. I was so thankful for such a thoughtful request. This is how that turned out:
My husband was waiting at the ambulance bay doors. He looked like he had been crying.
The ER
We were taken to an exam room and Greg was put on the bed. His face was tired. He was wide awake, but unable to speak.
We saw a doctor (and her same-named first-year medical student) almost right away. The doctor tried to ask him questions and run tests. I do not remember everything, but I do remember him not even looking at me when the doctor asked him who his mommy was and to point to her. I kept hugging him and putting my face really close to his. His response was to caress my arms and my face very gently, as he always does. Almost instinctively or reflexively. Without speaking, he seemed to remember his sweet loving nature.
We tried talking and singing, but he would not respond to us. He could look at us now, but no words came out.
The doctor must have explain what “post-ictal” state is, and expressed that this kind of length of time without speaking was not a usual symptom of a classif febrile seizure, and she would need the neurologist to come and evaluate him. This is the point where Steve and I almost lost it. He left the room and the doctor asked him if he was ok, he answered he was light headed, and I started to feel it too. Having has syncopes as a teenager, I knew what to do: I lied down on the filthy hospital emergency room floor and put my feet up. I remember Steve pointing at me and telling Greg “look how silly mommy is being!” and Greg looked at me. I smiled at him, but he didn’t smile back. That was the moment when Steve and I both realized Greg could be left with permanently damage, and it was too much to take.
Speech
It took Greg approximately 2 hours to recover his speech. At first he would only grunt/hum if he was asked a question, or he would press his lips together and blow through them (like a raspberry). He never cried. He simply could not talk.
Eventually he started saying “mamamamamamamamama.” It almost felt like he was learning to talk all over again, like a baby. I was right there with him and would just reply “baby baby baby…”
I have listened to enough podcasts about the brain to understand that songs and speech belong in different areas of the brain, so I started singing to him. At one point I sang to him and he responded:
ina: Watch me whip…
greg: whip.
ina: Watch me…
greg: nay nay
I was OVER THE MOON. He was speaking words! He wasn’t smiling or having fun, and he didn’t do it again even when I asked him to do it for daddy. But it was there! Then, when they put the IV in, he said “Ow Ow Ow!” which is what he normally says when something hurts. We had speech!
Slowly his words started coming back. Once he was able to ask me why we were here, I knew we were out of the woods. All I could think about in those moments was all those times I thought I had a perfect child, and how easily that could change.
By the time the neurologist saw him, he was already speaking. The neurologist believed the description of the seizure did not match with classic febrile seizure, and we needed an outpatient EEG to rule out epilepsy.

The Tests
Our doctor ordered the first set of tests: a CT scan of the head. They wanted to make sure there was no mass or bleeding. All clear.
Blood tests only revealed a slight increase in white blood cells, indicating there may be an infection somewhere. Now it was time to find the cause.
The doctor felt his stomach and thought she felt the liver being enlarged. Our handy family member pediatric nurse let the doctor know that he suffers from chronic constipation and it was possible that it was just poop pushing on the liver. The doctor felt it once more, and Greg said it hurt. Next test: x-ray to find out why the tummy was tender. All clear. Just poop mass. Liver was fine.
After the tests, Greg fell asleep. During his sleep, his oxygen levels dropped to 77 (other nurses saw it go down to 88, 84 and 82). The doctor wanted to admit him in case he could have a seizure in his sleep. We were put on a list to go up to a room.
The doctor now thought that perhaps he could have pneumonia. It would explain the shortness of breath. Greg had xrays on his chest. All clear.
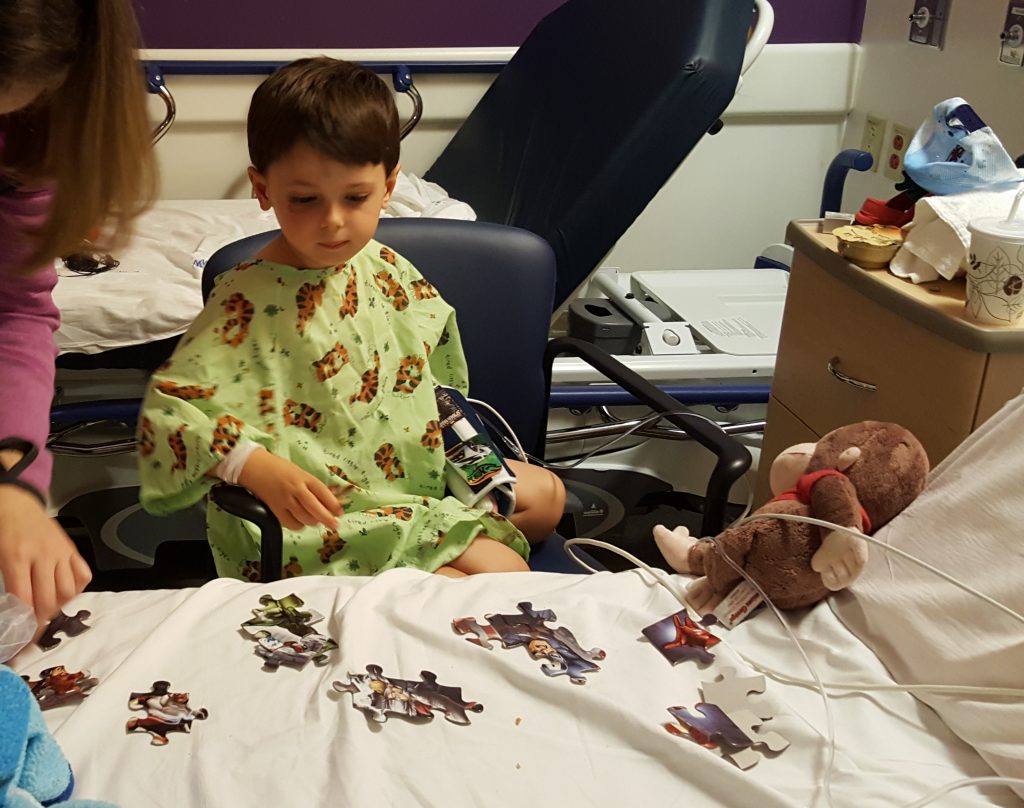
In the meantime, Greg spent time with his favorite people: mommy, daddy, nana, appa and auntie momo. We showed him videos, made a puzzle and he even got a DVD player from the ER to watch a Spider-Man movie.
The doctor thought of one more thing: intussusception. It’s a condition in which your intestine telescopes into itself, which is known to cause seizures. Greg was sent for an ultrasound. All clear.
They also tested Greg’s urine, but nothing came of it either.
By the time we got out of the ultrasound, it was 9:30pm. We finally made it to a room and were ready for bed by 11pm. Everyone went home but I stayed in a cot next to Greg.

The Emotional Turmoil
Both Steve and I had a moment of unrelated drama which set us off. Some time the next morning I went to the first floor to get a security badge. When I came back to the floor, I found that the door had a sign saying to try another door. But no other door seemed to go my way that would accept my badge. So I stood in front of the door staring at it and I started to bawl. Some guy found me there and helped me find someone who would let me back into the unit. I was crying inconsolably. I felt so fragile.
For Steve it was after we had been discharged and I told him I’d get him McDonalds. I had misunderstood him over the phone and didn’t get him a Coke. That was the last straw for him.
The Next Day
We met our doctors as soon as we got to the floor. Dr Zhu was very nice, as was Dr Raju (the one that took over for Dr Zhu in the morning). They explained everything to us step by step and did not make us feel stupid for asking the questions we were asking.
We asked why they didn’t do a lumbar puncture or a blood culture to rule out meningitis or a blood disorder. Answer: none of the tests indicate that Greg is actually sick, plus the fact that he has regained his old personality and is in good spirits indicates to them that there isn’t an underlying condition. What he had was probably caused by a virus. We should keep an eye on him until the virus goes away.
We were comfortable with the answers and took him home to recover.
The Day after Next
The day after the discharge Greg was still not keeping water or food down. We called his PCP and they recommended he go back to the ER if he hasn’t been able to keep food/drink down by 6pm.
Here’s Sunday’s log:
- 4:30am drink water, bloody nose (right side)
- 8 am drink water (multiple times)
- 8 am pipi
- 8:30 temp 99.5
- 8:30am throw up
- 9am tiny bite of toast, drink water
- 9:45 am throw up
- Refuses to eat
- Good spirits. Playing with dinosaurs.
- 10am temp 98
- 11am temp 98
- 11am eat pretzels
- 11:20 no throw up! Temp 98. Ritz crackers. Tiny bites.
- 11:40 stomach does not feel hard
- 12 had some pretzel bites
- 1pm down for a nap
- 3:30 awake from nap
- 4 lunch: sweet pot, chicken, bread
By 6pm, he was back to his old self. I showered him and noticed his arms were all skin and bones. I weighed him and he appeared to have lost 2 pounds (5% of his weight).
I decided to keep him home on Monday with me to keep watching him.
The End.
ina
")
